Chelation
|
|
June 30, 2019
Andrew Cutler Chelation Explained (8 EASY STEPS) By Paola Dziwetzki (Taken from YouTube) |
How To Chelate With The Andrew Cutler
Paola Dziwetzki | May 17, 2018 | 84 comments
Link: https://thepowerofozone.com/chelate-andrew-cutler-protocol/
1. The Andrew Cutler Protocol – Overview
IMPORTANT: Chelation can be performed only after ALL amalgam fillings and all other mercury sources have been removed. Chelating with amalgam leftovers can result in a mobilization and redistribution of mercury into the Central Nervous System. Please, ask your dentist for bite-wing x-rays to verify that you are truly amalgam free.
Chelating with the Andrew Cutler Protocol involves the following three chelators:
During the Andrew Cutler Chelation the chelators are taken in rounds of at least 63 hours in low oral dosages according to their half lives. After each round there is a break of at least three days.
What this means in practice is described in detail on this page.
Starting dosages range between 3 and 20 mg.
A successful chelation can take 100 to 300 rounds, or 1 to 5 years.
Table 1: Example of the constant succession of rounds and breaks during the Andrew Cutler program.
How To Chelate With The Andrew Cutler
Paola Dziwetzki | May 17, 2018 | 84 comments
Link: https://thepowerofozone.com/chelate-andrew-cutler-protocol/
1. The Andrew Cutler Protocol – Overview
IMPORTANT: Chelation can be performed only after ALL amalgam fillings and all other mercury sources have been removed. Chelating with amalgam leftovers can result in a mobilization and redistribution of mercury into the Central Nervous System. Please, ask your dentist for bite-wing x-rays to verify that you are truly amalgam free.
Chelating with the Andrew Cutler Protocol involves the following three chelators:
- ALA (Alpha Lipoic Acid), half life: 3 hours
- DMSA (Dimercaptosuccunic acid), half life: 3 to 4 hours
- DMPS (Dimercaptopropane sulfonic acid), half life: 6 to 8 hours
During the Andrew Cutler Chelation the chelators are taken in rounds of at least 63 hours in low oral dosages according to their half lives. After each round there is a break of at least three days.
What this means in practice is described in detail on this page.
Starting dosages range between 3 and 20 mg.
A successful chelation can take 100 to 300 rounds, or 1 to 5 years.
Table 1: Example of the constant succession of rounds and breaks during the Andrew Cutler program.

2. Chelating with DMSA
The purpose of DMSA is to lower mercury levels in the blood. In this way, it prepares the body for chelation with Alpha Lipoic Acid, which is the most important chelator.
DMSA is used during the first 3 months after the last mercury exposure, which in most cases is amalgam removal.
Chelating with DMSA: things to remember
You pick one dosage and stick to that dosage over the entire round. You select either a 3-hour or 4-hour interval. If you choose 3-hour intervals, then a DMSA round looks just like an ALA round (see table 5 or 6 below).
Table 2: Example of a round with DMSA with 4-hour intervals:
The purpose of DMSA is to lower mercury levels in the blood. In this way, it prepares the body for chelation with Alpha Lipoic Acid, which is the most important chelator.
DMSA is used during the first 3 months after the last mercury exposure, which in most cases is amalgam removal.
Chelating with DMSA: things to remember
- DMSA will clear mercury only out of the blood and the extracellular fluid. It cannot chelate mercury out of the brain or other organs.
- DMSA can be taken 4 days after mercury exposure has ended. For example: If you had your amalgams removed on May 1st, you can start using DMSA on May 5th.
- DMSA chelates mercury and lead.
- DMSA can lower neutrophils which can lead to a flare-up of candida.
- DMSA has a half life of 3 to 4 hours.
You pick one dosage and stick to that dosage over the entire round. You select either a 3-hour or 4-hour interval. If you choose 3-hour intervals, then a DMSA round looks just like an ALA round (see table 5 or 6 below).
Table 2: Example of a round with DMSA with 4-hour intervals:
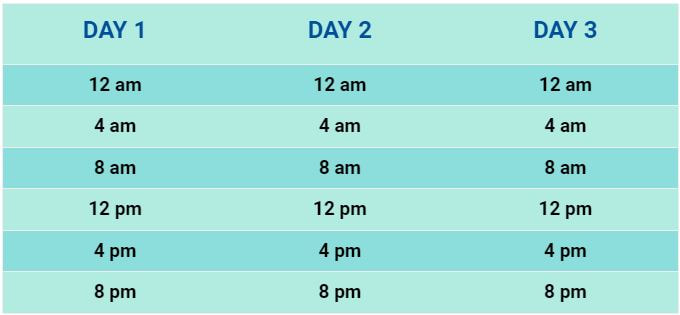
A 72 hours round with 4 hours intervals consists of 18 dosages. 72 hours / 4 hours intervals = 18. You can start a round at any random time. What is important that the intervals in between single dosages are always the same.
3. Chelating with DMPS
The purpose of DMPS is to lower mercury levels in the blood. It prepares the body for chelation with Alpha Lipoic Acid, which is the most important chelator.
DMPS is used during the first 3 months after the last mercury exposure has ended, which in most cases is amalgam removal.
Chelating with DMPS: things to remember
You pick one interval and dosage and stick to that interval over the entire round. So if you pick a 6-hour interval, you should keep that until the end of the round. Same if you pick a 8-hour interval. Do not change dosages mid-round.
Table 3: Example of a round with DMPS with 6-hour intervals.
The purpose of DMPS is to lower mercury levels in the blood. It prepares the body for chelation with Alpha Lipoic Acid, which is the most important chelator.
DMPS is used during the first 3 months after the last mercury exposure has ended, which in most cases is amalgam removal.
Chelating with DMPS: things to remember
- DMPS works very similarly to DMSA.
- According to Dr. Cutler, DMPS is not significantly more effective than DMSA, but most people tolerate it better than DMSA.
- DMPS will clear mercury only out of the blood and the extracellular fluid. It cannot chelate mercury out of the brain or organs.
- DMPS can be taken 4 days after mercury exposure has ended. In other words, if you had your amalgams removed on May 1st, you can start using DMPS on May 5th.
- Some people develop allergic reactions to the drug, which show up as rashes.
- DMPS is considerably more expensive than DMSA.
- DMPS chelates mercury and arsenic.
- DMPS has a half life of 6 to 8 hours.
You pick one interval and dosage and stick to that interval over the entire round. So if you pick a 6-hour interval, you should keep that until the end of the round. Same if you pick a 8-hour interval. Do not change dosages mid-round.
Table 3: Example of a round with DMPS with 6-hour intervals.
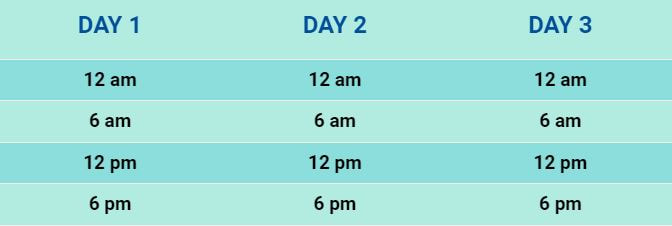
A 72 hours round with 6 hours intervals consists of 12 dosages. 72 hours / 6 hours intervals = 12. You can start a round at any random time. What is important that the intervals in between single dosages are always the same.
Table 4: Example of a round with DMPS with 8-hour intervals.
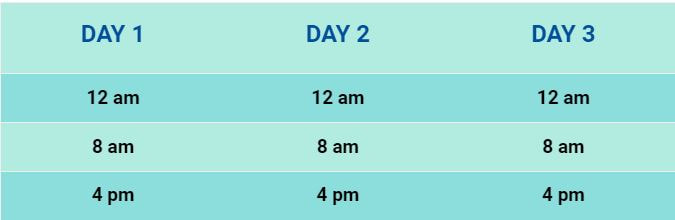
A 72 hours round with 6 hours intervals consists of 9 dosages. 72 hours / 8 hours intervals = 9. You can start a round at any random time. What is important that the intervals in between single dosages are always the same.
4. Chelating with ALA
Alpha Lipoic Acid is the most important chelator.
One can successfully chelate mercury with ALA alone. DMSA and DMPS are optional.
It’s the only one of the three agents which is able to penetrate the blood-brain barrier (BBB) and pull the mercury out of your Central Nervous System (CNS) and from the inside of your organs. You start chelating with ALA three months after the last mercury exposure.
Example: if you had your amalgams removed on Feb 1st, the earliest you can start chelating with ALA is May 1st.
Chelating with ALA: things to remember
You pick one dosage and keep that same dosage over the duration of the entire round. A round consists of minimum 63 hours.
Table 5: An example of a 63-hour round with ALA.
Alpha Lipoic Acid is the most important chelator.
One can successfully chelate mercury with ALA alone. DMSA and DMPS are optional.
It’s the only one of the three agents which is able to penetrate the blood-brain barrier (BBB) and pull the mercury out of your Central Nervous System (CNS) and from the inside of your organs. You start chelating with ALA three months after the last mercury exposure.
Example: if you had your amalgams removed on Feb 1st, the earliest you can start chelating with ALA is May 1st.
Chelating with ALA: things to remember
- ALA chelates mercury and arsenic.
- ALA has a half-life of 3 hours. This means that it must be taken every 3 hours, DAY and NIGHT. During the night, it’s possible to extend the intervals twice to 4 hours since the metabolism slows down when we sleep. During the day, you have to go back to 3-hour intervals.
You pick one dosage and keep that same dosage over the duration of the entire round. A round consists of minimum 63 hours.
Table 5: An example of a 63-hour round with ALA.
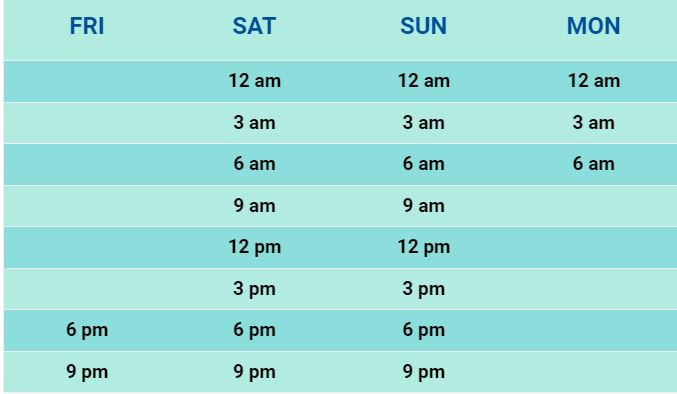
A 63 hours round with 3 hours intervals consists of 21 dosages. 63 hours / 3 hours intervals = 21. This example is ideal for people who work during the week or go to school. A 63 hours round as displayed above allows to start a round on Friday evening and finish Monday morning.
In this article I mostly choose 72-hour rounds simply because a) longer rounds are in general preferable to shorter ones; and b) if you want to always alternate 3 days on and 3 days off, then 72-hour rounds and 72-hour breaks make for a simple and clear schedule.
Table 6: An example of a 72-hour round with ALA.
Table 6: An example of a 72-hour round with ALA.
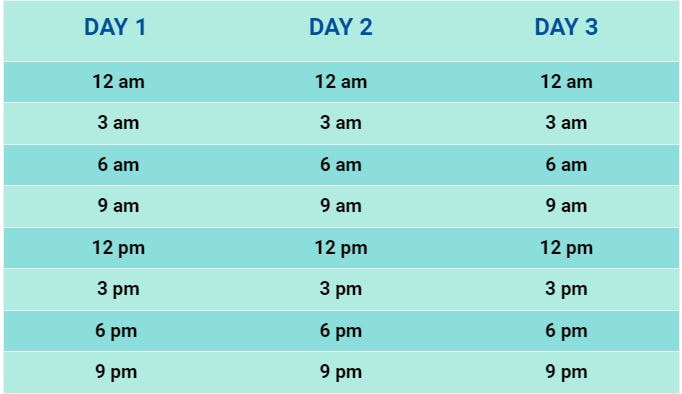
A 72-hour round consists of 24 dosages, or 8 per day: 72 hours / 3 hours intervals = 24 dosages.
5. Chelating with DMSA and ALA
The usual course of action is that people first get their amalgams removed, then chelate with DMSA or DMPS for 3 months to lower mercury blood levels, and after that add ALA.
But: If three or more than three months have passed since your last mercury exposure (in most cases in the form of amalgam fillings), you can start chelating with the combination of DMSA and ALA right away.
Example: If you had your amalgam fillings removed two years ago but you are learning about this protocol only now, you don’t have to chelate with DMSA first. You can immediately start with a combination of DMSA and ALA or ALA alone.
Practically speaking, in such a case it makes more sense to first start with just ALA to gauge one’s reaction and to see if there is a reaction at all. Then, once you have found a manageable amount of ALA for you, you can add DMSA at the same or half the dosage.
The ratio of ALA and DMSA is not very important for the success of the program. Ratios of around 1:1, 2:1 or 1:2 are common.
When DMSA and ALA are combined, you choose the half-life of 3 hours. That way, both compounds are taken together at the same time.
Table 7: An example of a 72-hour round with DMSA and ALA.
The usual course of action is that people first get their amalgams removed, then chelate with DMSA or DMPS for 3 months to lower mercury blood levels, and after that add ALA.
But: If three or more than three months have passed since your last mercury exposure (in most cases in the form of amalgam fillings), you can start chelating with the combination of DMSA and ALA right away.
Example: If you had your amalgam fillings removed two years ago but you are learning about this protocol only now, you don’t have to chelate with DMSA first. You can immediately start with a combination of DMSA and ALA or ALA alone.
Practically speaking, in such a case it makes more sense to first start with just ALA to gauge one’s reaction and to see if there is a reaction at all. Then, once you have found a manageable amount of ALA for you, you can add DMSA at the same or half the dosage.
The ratio of ALA and DMSA is not very important for the success of the program. Ratios of around 1:1, 2:1 or 1:2 are common.
When DMSA and ALA are combined, you choose the half-life of 3 hours. That way, both compounds are taken together at the same time.
Table 7: An example of a 72-hour round with DMSA and ALA.
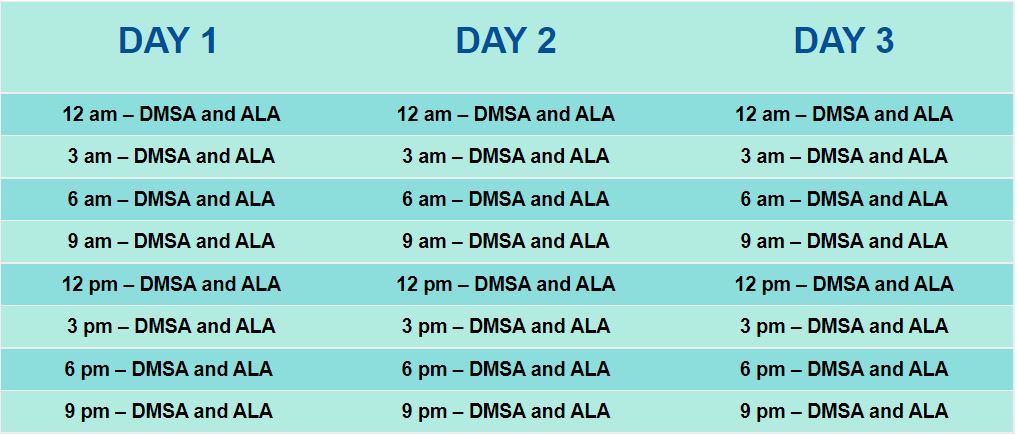
A 72-hour round consists of 24 ALA dosages and 12 DMPS dosages. ALA is taken every 3 hours, DMPS is taken every 6 hours. The exact starting time is irrelevant, it can be also 2:14 am on any day of the week. What is important are the constant intervals of 3 hours and 6 hours.
7. Choosing and increasing dosages
A recommended starting dosage is 3 mg to 20 mg. Some may need to go as low as 1 mg. Others can start with more than 20 mg.
Mercury chelation results in the controlled mobilisation of one of the most dangerous neurotoxins known to men. As a consequence symptoms can worsen or new symptoms can emerge during the protocol.
Dosages of the chelators are chosen in a way that symptoms during chelation remain manageable. You should be able to perform daily tasks while on round. If you feel unable to function, your dosage is too high.
In such a case, abort the round, wait at least 3 days and then start a new round at a lower dosage.
Alternatively, one can shorten the interval between the dosages. This often results in a more comfortable chelation experience.
Example: instead of taking ALA every 3 hours, you can take it every 2.5 hours.
Shorter intervals are allowed, longer ones are not (except twice at night).
At the beginning one should proceed with caution. The goal is to find the dosage where there is a reaction but it is tolerable. Until that dosage is found, one can increase by doubling the amount with each round.
Never change the dosage mid-round. Always wait for a new round to start on a higher (or lower) amount.
Once you have found the initial dosage for you, you stay there for several months before increasing by maximum 50%.
Example:
Round 1: 3 mg ALA.
No reaction. Neither on or off round.
Round 2: 6 mg ALA
No reaction. Neither on or off round.
Round 3: 12 mg ALA
No reaction. Neither on or off round.
Round 4: 25 mg ALA.
A distinct but still manageable reaction: improved fatigue on day 1, worse on day 2 on round. Pronounced irritability during the break.
Stay on the same dosage, 25 mg ALA, during rounds 5 to 12.
On round 12 there is as good as no discernible reaction in symptoms.
Round 13: 38 mg ALA (25 mg + 50% = 38 mg)
Again, there is a distinct but manageable reaction.
Continue doing rounds with 38 mg until there are no more reactions. Then increase again by maximum 50%.
Repeat this process again and again until you reach the maximum dosage of 3 mg of ALA per kg of body weight. So if you weigh 60 kg, your maximum dosage is 180 mg ALA.
It can take several years to reach one’s maximum dosage.
8. Dump Phase
The dump phase is a time period during mercury chelation when there is either no improvement or even a worsening of symptoms. It sets in around 2 to 4 months after starting chelation (or after amalgam removal). It shows its peak at around 6 to 9 months into chelation and can last several months.
Once the dump phase has passed, you’ll find that with continued chelation there will be a consistent improvement of your symptoms. The dump phase is only observed during mercury chelation. No other toxic metal shows this pattern.
It’s recommended that you chelate through the dump phase. Most people decide to reduce their chelator dosage during that time.
A recommended starting dosage is 3 mg to 20 mg. Some may need to go as low as 1 mg. Others can start with more than 20 mg.
Mercury chelation results in the controlled mobilisation of one of the most dangerous neurotoxins known to men. As a consequence symptoms can worsen or new symptoms can emerge during the protocol.
Dosages of the chelators are chosen in a way that symptoms during chelation remain manageable. You should be able to perform daily tasks while on round. If you feel unable to function, your dosage is too high.
In such a case, abort the round, wait at least 3 days and then start a new round at a lower dosage.
Alternatively, one can shorten the interval between the dosages. This often results in a more comfortable chelation experience.
Example: instead of taking ALA every 3 hours, you can take it every 2.5 hours.
Shorter intervals are allowed, longer ones are not (except twice at night).
At the beginning one should proceed with caution. The goal is to find the dosage where there is a reaction but it is tolerable. Until that dosage is found, one can increase by doubling the amount with each round.
Never change the dosage mid-round. Always wait for a new round to start on a higher (or lower) amount.
Once you have found the initial dosage for you, you stay there for several months before increasing by maximum 50%.
Example:
Round 1: 3 mg ALA.
No reaction. Neither on or off round.
Round 2: 6 mg ALA
No reaction. Neither on or off round.
Round 3: 12 mg ALA
No reaction. Neither on or off round.
Round 4: 25 mg ALA.
A distinct but still manageable reaction: improved fatigue on day 1, worse on day 2 on round. Pronounced irritability during the break.
Stay on the same dosage, 25 mg ALA, during rounds 5 to 12.
On round 12 there is as good as no discernible reaction in symptoms.
Round 13: 38 mg ALA (25 mg + 50% = 38 mg)
Again, there is a distinct but manageable reaction.
Continue doing rounds with 38 mg until there are no more reactions. Then increase again by maximum 50%.
Repeat this process again and again until you reach the maximum dosage of 3 mg of ALA per kg of body weight. So if you weigh 60 kg, your maximum dosage is 180 mg ALA.
It can take several years to reach one’s maximum dosage.
8. Dump Phase
The dump phase is a time period during mercury chelation when there is either no improvement or even a worsening of symptoms. It sets in around 2 to 4 months after starting chelation (or after amalgam removal). It shows its peak at around 6 to 9 months into chelation and can last several months.
Once the dump phase has passed, you’ll find that with continued chelation there will be a consistent improvement of your symptoms. The dump phase is only observed during mercury chelation. No other toxic metal shows this pattern.
It’s recommended that you chelate through the dump phase. Most people decide to reduce their chelator dosage during that time.
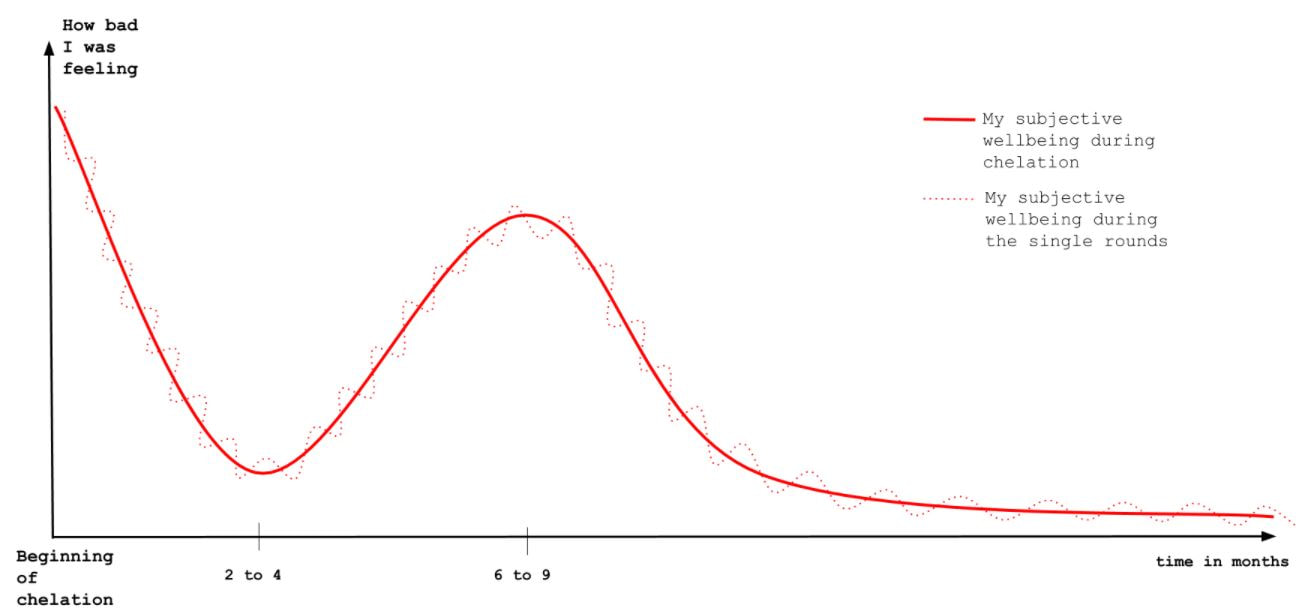
This is an approximate illustration of what I went through during the first months of chelation. I started the AC program in September 2013, experienced an improvement in symptoms during the first 2 to 3 months, after which progress seemed to have stalled. By March/April 2014 I was doing very poorly with new, troubling symptoms setting in. I was feeling so bad that I had stopped chelating during that time. This was, unbeknownst to me at that time, the peak of the dump phase. Dr. Cutler maintains that the dump phase is something that most people go through while detoxing mercury.
9. Supplements
Dr. Andrew Cutler called the following supplements the “Core Four”. They are the most important supplements to take during chelation. Minerals and vitamins speed up recovery and allow the body to fix the damage mercury has caused.
1. Vitamin C*, 2 to 5 grams per day. Or more if bowel tolerance allows.
2. Magnesium, up to 1,000 mg per day. Take it in smaller dosages of 150 to 200 mg with meals and before bed time.
3. Zinc, 25 to 50 mg per day
4. Vitamin E, up to 1,000 IE per day.
* A word of caution about Vitamin C. This is a personal note of mine and is a strict deviation from the Cutler protocol. I have successfully chelated without supplementing with Vitamin C (or zinc or Vitamin E). The reason I did that was because I reacted badly to it and to most other supplements. As I later found out this was due to oxalates. Dr. Cutler maintains that the idea of oxalates causing problems is nonsense. After visits to ER and numerous doctors, I had to find out that he was dead wrong about it. Vitamin C can convert to oxalates in the body. If there are significant oxalate stores present, taking Vitamin C in large dosages can be highly detrimental to one’s health, even without kidney problems.
There are also many other supplements which are recommended. The most popular ones are Adrenal Cortex and B Vitamins. According to Dr. Cutler anything that will lessen symptoms and make chelation more bearable should be taken. This includes pharmaceuticals and even psychotropic drugs.
10. My experience with the Andrew Cutler Chelation
From September 2013 until February 2018, I chelated with the Andrew Cutler protocol in order to remedy a chronic mercury poisoning. Except for a 1.5 month break in March/April 2014, I chelated continuously during that time, only taking the minimum 3-day breaks in between rounds.
During that period I have performed over 211 rounds from 3 days to 78 days in length. I have reached dosages of up to 400 mg ALA. In order to be officially finished, I would need to chelate for another 30 days. But I consider myself as basically being mercury-free at this point.
At the end of 2014 I have completed a one-on-one online / phone course with Dr. Andrew Cutler. After having successfully passed the exam, I was issued a certificate.
This, plus my 4 year ACC experience, makes me a certified Cutler expert.
11. What does mercury chelation have to do with ozone therapy? Why am I writing about chelation at all here? Isn’t this an ozone website?
I am of the opinion that a large number of people who do ozone treatments for infections like Lyme or inflammatory conditions like MS, really may be dealing with a misdiagnosed mercury poisoning. Ozone is not able to remove mercury.
Unless mercury is detoxed properly, antibiotics or even ozone therapy, may not work as intended.
Hence, getting rid of this most insidious of toxins is of paramount importance on the way to health.
Although I had to find out that Andrew Cutler was wrong about a number of things, the most important one being oxalates (more on that in a future article), I do believe that when it comes to mercury removal his approach is the only scientifically sound and is the safest way to remove the toxic metal from deep stores like brain, liver, or adrenals.
Recommended reading: “Amalgam Illness”, Andrew Hall Cutler, PhD
9. Supplements
Dr. Andrew Cutler called the following supplements the “Core Four”. They are the most important supplements to take during chelation. Minerals and vitamins speed up recovery and allow the body to fix the damage mercury has caused.
1. Vitamin C*, 2 to 5 grams per day. Or more if bowel tolerance allows.
2. Magnesium, up to 1,000 mg per day. Take it in smaller dosages of 150 to 200 mg with meals and before bed time.
3. Zinc, 25 to 50 mg per day
4. Vitamin E, up to 1,000 IE per day.
* A word of caution about Vitamin C. This is a personal note of mine and is a strict deviation from the Cutler protocol. I have successfully chelated without supplementing with Vitamin C (or zinc or Vitamin E). The reason I did that was because I reacted badly to it and to most other supplements. As I later found out this was due to oxalates. Dr. Cutler maintains that the idea of oxalates causing problems is nonsense. After visits to ER and numerous doctors, I had to find out that he was dead wrong about it. Vitamin C can convert to oxalates in the body. If there are significant oxalate stores present, taking Vitamin C in large dosages can be highly detrimental to one’s health, even without kidney problems.
There are also many other supplements which are recommended. The most popular ones are Adrenal Cortex and B Vitamins. According to Dr. Cutler anything that will lessen symptoms and make chelation more bearable should be taken. This includes pharmaceuticals and even psychotropic drugs.
10. My experience with the Andrew Cutler Chelation
From September 2013 until February 2018, I chelated with the Andrew Cutler protocol in order to remedy a chronic mercury poisoning. Except for a 1.5 month break in March/April 2014, I chelated continuously during that time, only taking the minimum 3-day breaks in between rounds.
During that period I have performed over 211 rounds from 3 days to 78 days in length. I have reached dosages of up to 400 mg ALA. In order to be officially finished, I would need to chelate for another 30 days. But I consider myself as basically being mercury-free at this point.
At the end of 2014 I have completed a one-on-one online / phone course with Dr. Andrew Cutler. After having successfully passed the exam, I was issued a certificate.
This, plus my 4 year ACC experience, makes me a certified Cutler expert.
11. What does mercury chelation have to do with ozone therapy?
Why am I writing about chelation at all here? Isn’t this an ozone website?
I am of the opinion that a large number of people who do ozone treatments for infections like Lyme or inflammatory conditions like MS, really may be dealing with a misdiagnosed mercury poisoning. Ozone is not able to remove mercury.
Unless mercury is detoxed properly, antibiotics or even ozone therapy, may not work as intended.
Hence, getting rid of this most insidious of toxins is of paramount importance on the way to health.
Although I had to find out that Andrew Cutler was wrong about a number of things, the most important one being oxalates (more on that in a future article), I do believe that when it comes to mercury removal his approach is the only scientifically sound and is the safest way to remove the toxic metal from deep stores like brain, liver, or adrenals.
Recommended reading: “Amalgam Illness”, Andrew Hall Cutler, PhD
Dr. Andrew Cutler called the following supplements the “Core Four”. They are the most important supplements to take during chelation. Minerals and vitamins speed up recovery and allow the body to fix the damage mercury has caused.
1. Vitamin C*, 2 to 5 grams per day. Or more if bowel tolerance allows.
2. Magnesium, up to 1,000 mg per day. Take it in smaller dosages of 150 to 200 mg with meals and before bed time.
3. Zinc, 25 to 50 mg per day
4. Vitamin E, up to 1,000 IE per day.
* A word of caution about Vitamin C. This is a personal note of mine and is a strict deviation from the Cutler protocol. I have successfully chelated without supplementing with Vitamin C (or zinc or Vitamin E). The reason I did that was because I reacted badly to it and to most other supplements. As I later found out this was due to oxalates. Dr. Cutler maintains that the idea of oxalates causing problems is nonsense. After visits to ER and numerous doctors, I had to find out that he was dead wrong about it. Vitamin C can convert to oxalates in the body. If there are significant oxalate stores present, taking Vitamin C in large dosages can be highly detrimental to one’s health, even without kidney problems.
There are also many other supplements which are recommended. The most popular ones are Adrenal Cortex and B Vitamins. According to Dr. Cutler anything that will lessen symptoms and make chelation more bearable should be taken. This includes pharmaceuticals and even psychotropic drugs.
10. My experience with the Andrew Cutler Chelation
From September 2013 until February 2018, I chelated with the Andrew Cutler protocol in order to remedy a chronic mercury poisoning. Except for a 1.5 month break in March/April 2014, I chelated continuously during that time, only taking the minimum 3-day breaks in between rounds.
During that period I have performed over 211 rounds from 3 days to 78 days in length. I have reached dosages of up to 400 mg ALA. In order to be officially finished, I would need to chelate for another 30 days. But I consider myself as basically being mercury-free at this point.
At the end of 2014 I have completed a one-on-one online / phone course with Dr. Andrew Cutler. After having successfully passed the exam, I was issued a certificate.
This, plus my 4 year ACC experience, makes me a certified Cutler expert.
11. What does mercury chelation have to do with ozone therapy? Why am I writing about chelation at all here? Isn’t this an ozone website?
I am of the opinion that a large number of people who do ozone treatments for infections like Lyme or inflammatory conditions like MS, really may be dealing with a misdiagnosed mercury poisoning. Ozone is not able to remove mercury.
Unless mercury is detoxed properly, antibiotics or even ozone therapy, may not work as intended.
Hence, getting rid of this most insidious of toxins is of paramount importance on the way to health.
Although I had to find out that Andrew Cutler was wrong about a number of things, the most important one being oxalates (more on that in a future article), I do believe that when it comes to mercury removal his approach is the only scientifically sound and is the safest way to remove the toxic metal from deep stores like brain, liver, or adrenals.
Recommended reading: “Amalgam Illness”, Andrew Hall Cutler, PhD
9. Supplements
Dr. Andrew Cutler called the following supplements the “Core Four”. They are the most important supplements to take during chelation. Minerals and vitamins speed up recovery and allow the body to fix the damage mercury has caused.
1. Vitamin C*, 2 to 5 grams per day. Or more if bowel tolerance allows.
2. Magnesium, up to 1,000 mg per day. Take it in smaller dosages of 150 to 200 mg with meals and before bed time.
3. Zinc, 25 to 50 mg per day
4. Vitamin E, up to 1,000 IE per day.
* A word of caution about Vitamin C. This is a personal note of mine and is a strict deviation from the Cutler protocol. I have successfully chelated without supplementing with Vitamin C (or zinc or Vitamin E). The reason I did that was because I reacted badly to it and to most other supplements. As I later found out this was due to oxalates. Dr. Cutler maintains that the idea of oxalates causing problems is nonsense. After visits to ER and numerous doctors, I had to find out that he was dead wrong about it. Vitamin C can convert to oxalates in the body. If there are significant oxalate stores present, taking Vitamin C in large dosages can be highly detrimental to one’s health, even without kidney problems.
There are also many other supplements which are recommended. The most popular ones are Adrenal Cortex and B Vitamins. According to Dr. Cutler anything that will lessen symptoms and make chelation more bearable should be taken. This includes pharmaceuticals and even psychotropic drugs.
10. My experience with the Andrew Cutler Chelation
From September 2013 until February 2018, I chelated with the Andrew Cutler protocol in order to remedy a chronic mercury poisoning. Except for a 1.5 month break in March/April 2014, I chelated continuously during that time, only taking the minimum 3-day breaks in between rounds.
During that period I have performed over 211 rounds from 3 days to 78 days in length. I have reached dosages of up to 400 mg ALA. In order to be officially finished, I would need to chelate for another 30 days. But I consider myself as basically being mercury-free at this point.
At the end of 2014 I have completed a one-on-one online / phone course with Dr. Andrew Cutler. After having successfully passed the exam, I was issued a certificate.
This, plus my 4 year ACC experience, makes me a certified Cutler expert.
11. What does mercury chelation have to do with ozone therapy?
Why am I writing about chelation at all here? Isn’t this an ozone website?
I am of the opinion that a large number of people who do ozone treatments for infections like Lyme or inflammatory conditions like MS, really may be dealing with a misdiagnosed mercury poisoning. Ozone is not able to remove mercury.
Unless mercury is detoxed properly, antibiotics or even ozone therapy, may not work as intended.
Hence, getting rid of this most insidious of toxins is of paramount importance on the way to health.
Although I had to find out that Andrew Cutler was wrong about a number of things, the most important one being oxalates (more on that in a future article), I do believe that when it comes to mercury removal his approach is the only scientifically sound and is the safest way to remove the toxic metal from deep stores like brain, liver, or adrenals.
Recommended reading: “Amalgam Illness”, Andrew Hall Cutler, PhD
|
|
October 3, 2019
ANDREW CUTLER CHELATION: How to make small dosages with a capsule machine (STEP BY STEP)By Paola Dziwetzki (Taken from YouTube |
